It doesn't end there. In a third study, the researchers contrived to influence beliefs about self-control by giving student smokers a bogus implicit test of impulse control. Later, the students were challenged to watch the film "Coffee and Cigarettes" whilst abstaining from smoking. They were promised a greater cash reward the more difficult they made the challenge for themselves. In this case, students given bogus test feedback indicating they had high self-control were more likely to opt for greater temptation - holding the cigarette in their hand rather than having it on the desk - and they were more likely to give in to that temptation.
Finally, Nordgren's team tested the idea that "restraint bias" could explain why drug addicts are so prone to relapse. They recruited 55 participants through a smoking-cessation programme, all of whom had been smoke free for at least three weeks. Those who said they had more impulse control also tended to say they wouldn't be trying so hard to avoid temptation, such as the company of other smokers. Four months' later, those with the inflated sense of impulse control were more likely to have relapsed.
"The restraint bias suggests that people are willing to experiment with addictive drugs simply because they believe they can overcome the addiction," the researchers said. "An urgent task for future research is to test whether enduring shifts in impulse-control beliefs can be created."
Saturday, December 19, 2009
The dangers of overconfidence
Support for twelve-step programs' emphasis on powerlessness?
Friday, December 18, 2009
Who me?
Discouraging news in terms of attraction to treatment:
A lack of perceived need for treatment is still a key reason for the low rate of treatment in people with alcohol-use disorder and for the lack of progress in reducing the scale of this problem, according to an analysis of recent large surveys in the United States.This is an important challenge for providers. How do we attract people who are not coerced and/or late stage? It's time for providers to take responsibility for this.
In the National Survey on Drug Use and Health (NSDUH) dataset, 7,009 respondents met the diagnostic criteria for an alcohol-use disorder (dependence or abuse), among whom 89.6 percent said they did not perceive a need for treatment or counseling for their alcohol use in the prior 12 months. In the 3,305 participants in the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) who met the criteria for alcohol-use disorder, a similar rate of 89 percent said they did not think they needed treatment for alcohol-use treatment.
It would be more meaningful if they separated dependence and abuse.
What happens when free treatment is offered?
Early returns from a Massachusetts initiative offering free smoking cessation treatment:
When Massachusetts began offering virtually free treatments to help poor residents of the state stop smoking in 2006, proponents hoped the new Medicaid program would someday reap benefits.
But state officials never expected it would happen so soon.
New state data show a steep drop in the smoking rate among poor people. When the program started, about 38 percent of poor Massachusetts residents smoked. By 2008, the smoking rate for poor residents had dropped to about 28 percent, a decrease of about 30,000 people in two and a half years, or one in six smokers, said Lois Keithly, director of the state’s Tobacco Cessation and Prevention Program.
There are also indications that the drop has lowered rates of hospitalization for heart attacks and emergency room visits for asthma attacks, she said.
The data has not yet been peer-reviewed. But the numbers have already grabbed national attention, with several United States senators and antismoking advocates using the data to push for similar new Medicaid coverage for tobacco addiction in the national health care legislation.
Mental-health parity laws require oversight
Findings from the implementation of mental health parity in California:
- Costs associated with parity were in line with, or even below, the projections.
- Most health plans responded to the parity law by lifting limits on the annual number of days allowed for inpatient treatments and the number of visits allowed for outpatient treatment.
- Concerns arose over the use of "medical necessity" clauses to authorize treatments and control costs. Medical necessity is typically defined as the need to supply a service for a condition that could endanger life or cause significant illness, suffering or disability and for which there is no adequate, less costly alternative available.
- Consumers also complained about being referred to lists of mental-health providers only to find out that providers on the list were not taking new patients.
- Health insurance providers felt the list of diagnoses covered under the parity law was arbitrary in excluding certain diagnoses.
- Some doctors reported that they chose a parity diagnosis for a patient in order to ensure insurance coverage although it wasn't the most accurate diagnosis. Some doctors said they had little flexibility to change a client's diagnosis if he or she improved because they believed the health plan would then stop providing coverage for continuing care or care for a lesser diagnosis.
- Nearly half of Californians polled in focus groups were unaware of the parity law.
Wednesday, December 16, 2009
an abuse of human rights
An opinion piece in the Guardian makes a powerful indictment of the use of methadone in U.K. prisons. (I'm not clear whether the controversy is about methadone maintenance or methadone detox in prisons. I see both referenced.)
In a jail recently, I watched a slow, shuffling queue of men in the rain. The sight of these addicts lining up outside the dispensary for their drugs must be one of the saddest and most shameful in our prison estate, yet giving them drugs is now the cornerstone of policy throughout western Europe – the argument being that we should accept that the addicted will always be with us and, instead of trying to change them, we should limit the damage they can do to society. Just get them on a programme of controlled drug use and the public will be protected from the crime and chaos that are the bedfellows of addiction.It seems that recovery could offer an organizing paradigm to diffuse some of the tension here. If the MMTs in question adopted a recovery-oriented approach and evaluated themselves with recovery-oriented outcomes, it might offer a path to progress in this dispute.
...
Maybe you have to live with your own addiction and go through the various methods of so-called treatment to understand the truth: that the methadone programme is an abuse of human rights. Every addict should be given the chance to recover. Most addicts do not believe it is possible to lead a fulfilling and drugs-free life. Their world is out of control and underpinned by the belief that they must commit crime to get drugs, or wait for the doctor to hand them over. It is shameful that our public services reinforce this view, instead of giving individuals the help they need to change.
Monday, December 14, 2009
Less harmful than alcohol?!?!
 The Boston Globe offers a good summary of the recent U.K. row over drug classification:
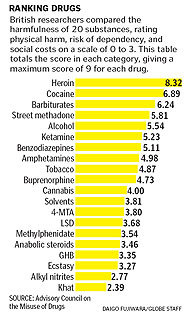
The Boston Globe offers a good summary of the recent U.K. row over drug classification:In the long and tortured debate over drug policy, one of the strangest episodes has been playing out this fall in the United Kingdom, where the country’s top drug adviser was recently fired for publicly criticizing his own government’s drug laws....The list, printed as a chart with the unassuming title “Mean Harm Scores for 20 Substances,” ranked a set of common drugs, both legal and illegal, in order of their harmfulness - how addictive they were, how physically damaging, and how much they threatened society. Many drug specialists now consider it one of the most objective sources available on the actual harmfulness of different substances.
That ranking showed, with numbers, what Nutt was fired for saying out loud: Overall, alcohol is far worse than many illegal drugs. So is tobacco. Smoking pot is less harmful than drinking, and LSD is less damaging yet.
Saturday, December 12, 2009
Poor Children Likelier to Get Antipsychotics
Troubling news for poor kids with emotional/behavior problems:
New federally financed drug research reveals a stark disparity: children covered by Medicaid are given powerful antipsychotic medicines at a rate four times higher than children whose parents have private insurance. And the Medicaid children are more likely to receive the drugs for less severe conditions than their middle-class counterparts, the data shows.
Thursday, December 10, 2009
A. Thomas McLellan
I had no idea that McLellan has been so personally affected by addiction:

But the loss of his younger son, who overdosed on anti-anxiety medication and Scotch last year at age 30 while his older son was in residential treatment for alcoholism and cocaine addiction, changed his perspective.
“That’s why I took this job,” said Dr. McLellan, who was sworn in as the deputy director of the Office of National Drug Control Policy in August. “I thought it was some kind of sign, you know. I would never have done it. I loved all the people I’ve worked with, I loved my life. But I thought maybe there’s a way where what I know plus what I feel could make a difference.”
Married to a recovering cocaine addict, Dr. McLellan has been engulfed by addiction in life and work. His own family has been a personal battleground for one of the country’s most complex and entrenched problems, while as an expert he has been a leading voice for the idea that addiction is a chronic illness and not a moral issue.
Sunday, December 06, 2009
Gradualism
Addiction Professional shines a light on Scott Kellogg and his Gradualism model. I've mentioned him several times in this blog and he has been kind enough to link to me on his website.
Two months ago Kellogg established a website (http://gradualismandaddiction.org) that he hopes will serve as a vehicle for discussion around a more nuanced approach to treatment. He says that after he began using the term “gradualism,” he noticed that practitioners in non-abstinence based initiatives in Europe in the 1970s had used the term “gradual change” to describe what they were trying to instill in persons with substance use problems.
A Gestalt-trained therapist, Kellogg holds some views that seem to place him closer to the harm reductionist’s way of looking at substance use and recovery. He questions treatment center practices that appear to profess abstinence at the risk of losing many clients before they can start making progress. He states his belief that “there’s a crisis in our treatment world because many people don’t like treatment.”
Yet he also says his perspective goes against the tenets held by many harm reductionists. He is most impatient with the attitude in some needle exchange programs and similar initiatives that “we would never tell people what to do.” Offering a shower, a sandwich and a clean needle and then repeating the process time and again are fine in the short term, but at some point you need to help build a life after you’ve saved one, he suggests.

Subscribe to:
Comments (Atom)