It doesn't end there. In a third study, the researchers contrived to influence beliefs about self-control by giving student smokers a bogus implicit test of impulse control. Later, the students were challenged to watch the film "Coffee and Cigarettes" whilst abstaining from smoking. They were promised a greater cash reward the more difficult they made the challenge for themselves. In this case, students given bogus test feedback indicating they had high self-control were more likely to opt for greater temptation - holding the cigarette in their hand rather than having it on the desk - and they were more likely to give in to that temptation.
Finally, Nordgren's team tested the idea that "restraint bias" could explain why drug addicts are so prone to relapse. They recruited 55 participants through a smoking-cessation programme, all of whom had been smoke free for at least three weeks. Those who said they had more impulse control also tended to say they wouldn't be trying so hard to avoid temptation, such as the company of other smokers. Four months' later, those with the inflated sense of impulse control were more likely to have relapsed.
"The restraint bias suggests that people are willing to experiment with addictive drugs simply because they believe they can overcome the addiction," the researchers said. "An urgent task for future research is to test whether enduring shifts in impulse-control beliefs can be created."
Saturday, December 19, 2009
The dangers of overconfidence
Support for twelve-step programs' emphasis on powerlessness?
Friday, December 18, 2009
Who me?
Discouraging news in terms of attraction to treatment:
A lack of perceived need for treatment is still a key reason for the low rate of treatment in people with alcohol-use disorder and for the lack of progress in reducing the scale of this problem, according to an analysis of recent large surveys in the United States.This is an important challenge for providers. How do we attract people who are not coerced and/or late stage? It's time for providers to take responsibility for this.
In the National Survey on Drug Use and Health (NSDUH) dataset, 7,009 respondents met the diagnostic criteria for an alcohol-use disorder (dependence or abuse), among whom 89.6 percent said they did not perceive a need for treatment or counseling for their alcohol use in the prior 12 months. In the 3,305 participants in the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) who met the criteria for alcohol-use disorder, a similar rate of 89 percent said they did not think they needed treatment for alcohol-use treatment.
It would be more meaningful if they separated dependence and abuse.
What happens when free treatment is offered?
Early returns from a Massachusetts initiative offering free smoking cessation treatment:
When Massachusetts began offering virtually free treatments to help poor residents of the state stop smoking in 2006, proponents hoped the new Medicaid program would someday reap benefits.
But state officials never expected it would happen so soon.
New state data show a steep drop in the smoking rate among poor people. When the program started, about 38 percent of poor Massachusetts residents smoked. By 2008, the smoking rate for poor residents had dropped to about 28 percent, a decrease of about 30,000 people in two and a half years, or one in six smokers, said Lois Keithly, director of the state’s Tobacco Cessation and Prevention Program.
There are also indications that the drop has lowered rates of hospitalization for heart attacks and emergency room visits for asthma attacks, she said.
The data has not yet been peer-reviewed. But the numbers have already grabbed national attention, with several United States senators and antismoking advocates using the data to push for similar new Medicaid coverage for tobacco addiction in the national health care legislation.
Mental-health parity laws require oversight
Findings from the implementation of mental health parity in California:
- Costs associated with parity were in line with, or even below, the projections.
- Most health plans responded to the parity law by lifting limits on the annual number of days allowed for inpatient treatments and the number of visits allowed for outpatient treatment.
- Concerns arose over the use of "medical necessity" clauses to authorize treatments and control costs. Medical necessity is typically defined as the need to supply a service for a condition that could endanger life or cause significant illness, suffering or disability and for which there is no adequate, less costly alternative available.
- Consumers also complained about being referred to lists of mental-health providers only to find out that providers on the list were not taking new patients.
- Health insurance providers felt the list of diagnoses covered under the parity law was arbitrary in excluding certain diagnoses.
- Some doctors reported that they chose a parity diagnosis for a patient in order to ensure insurance coverage although it wasn't the most accurate diagnosis. Some doctors said they had little flexibility to change a client's diagnosis if he or she improved because they believed the health plan would then stop providing coverage for continuing care or care for a lesser diagnosis.
- Nearly half of Californians polled in focus groups were unaware of the parity law.
Wednesday, December 16, 2009
an abuse of human rights
An opinion piece in the Guardian makes a powerful indictment of the use of methadone in U.K. prisons. (I'm not clear whether the controversy is about methadone maintenance or methadone detox in prisons. I see both referenced.)
In a jail recently, I watched a slow, shuffling queue of men in the rain. The sight of these addicts lining up outside the dispensary for their drugs must be one of the saddest and most shameful in our prison estate, yet giving them drugs is now the cornerstone of policy throughout western Europe – the argument being that we should accept that the addicted will always be with us and, instead of trying to change them, we should limit the damage they can do to society. Just get them on a programme of controlled drug use and the public will be protected from the crime and chaos that are the bedfellows of addiction.It seems that recovery could offer an organizing paradigm to diffuse some of the tension here. If the MMTs in question adopted a recovery-oriented approach and evaluated themselves with recovery-oriented outcomes, it might offer a path to progress in this dispute.
...
Maybe you have to live with your own addiction and go through the various methods of so-called treatment to understand the truth: that the methadone programme is an abuse of human rights. Every addict should be given the chance to recover. Most addicts do not believe it is possible to lead a fulfilling and drugs-free life. Their world is out of control and underpinned by the belief that they must commit crime to get drugs, or wait for the doctor to hand them over. It is shameful that our public services reinforce this view, instead of giving individuals the help they need to change.
Monday, December 14, 2009
Less harmful than alcohol?!?!
 The Boston Globe offers a good summary of the recent U.K. row over drug classification:
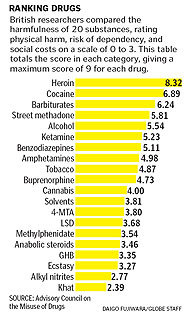
The Boston Globe offers a good summary of the recent U.K. row over drug classification:In the long and tortured debate over drug policy, one of the strangest episodes has been playing out this fall in the United Kingdom, where the country’s top drug adviser was recently fired for publicly criticizing his own government’s drug laws....The list, printed as a chart with the unassuming title “Mean Harm Scores for 20 Substances,” ranked a set of common drugs, both legal and illegal, in order of their harmfulness - how addictive they were, how physically damaging, and how much they threatened society. Many drug specialists now consider it one of the most objective sources available on the actual harmfulness of different substances.
That ranking showed, with numbers, what Nutt was fired for saying out loud: Overall, alcohol is far worse than many illegal drugs. So is tobacco. Smoking pot is less harmful than drinking, and LSD is less damaging yet.
Saturday, December 12, 2009
Poor Children Likelier to Get Antipsychotics
Troubling news for poor kids with emotional/behavior problems:
New federally financed drug research reveals a stark disparity: children covered by Medicaid are given powerful antipsychotic medicines at a rate four times higher than children whose parents have private insurance. And the Medicaid children are more likely to receive the drugs for less severe conditions than their middle-class counterparts, the data shows.
Thursday, December 10, 2009
A. Thomas McLellan
I had no idea that McLellan has been so personally affected by addiction:

But the loss of his younger son, who overdosed on anti-anxiety medication and Scotch last year at age 30 while his older son was in residential treatment for alcoholism and cocaine addiction, changed his perspective.
“That’s why I took this job,” said Dr. McLellan, who was sworn in as the deputy director of the Office of National Drug Control Policy in August. “I thought it was some kind of sign, you know. I would never have done it. I loved all the people I’ve worked with, I loved my life. But I thought maybe there’s a way where what I know plus what I feel could make a difference.”
Married to a recovering cocaine addict, Dr. McLellan has been engulfed by addiction in life and work. His own family has been a personal battleground for one of the country’s most complex and entrenched problems, while as an expert he has been a leading voice for the idea that addiction is a chronic illness and not a moral issue.
Sunday, December 06, 2009
Gradualism
Addiction Professional shines a light on Scott Kellogg and his Gradualism model. I've mentioned him several times in this blog and he has been kind enough to link to me on his website.
Two months ago Kellogg established a website (http://gradualismandaddiction.org) that he hopes will serve as a vehicle for discussion around a more nuanced approach to treatment. He says that after he began using the term “gradualism,” he noticed that practitioners in non-abstinence based initiatives in Europe in the 1970s had used the term “gradual change” to describe what they were trying to instill in persons with substance use problems.
A Gestalt-trained therapist, Kellogg holds some views that seem to place him closer to the harm reductionist’s way of looking at substance use and recovery. He questions treatment center practices that appear to profess abstinence at the risk of losing many clients before they can start making progress. He states his belief that “there’s a crisis in our treatment world because many people don’t like treatment.”
Yet he also says his perspective goes against the tenets held by many harm reductionists. He is most impatient with the attitude in some needle exchange programs and similar initiatives that “we would never tell people what to do.” Offering a shower, a sandwich and a clean needle and then repeating the process time and again are fine in the short term, but at some point you need to help build a life after you’ve saved one, he suggests.

Monday, November 09, 2009
Tab dump
- Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence - The metareview notes that there were few attempts to measure improvements in wellbeing.
- Alcohol-Induced Blackout - Are they predictive of dependence?
- Parity to Become Federal Law Despite Rule-Making Delay
- Policies to Prevent Drug Problems: A Research Agenda for 2010-2015 - Robert Wood Johnson's research agenda
Friday, November 06, 2009
Stigma and community
I read this Ta-Nehisi Coates post yesterday on domestic violence, responsibility, individual agency, community, shame, isolation and empowerment. It's really stuck with me. Very heavy, heady stuff in a very short post.
It got me thinking about some of the mechanisms of addiction and stigma, and the healing mechanisms of the recovering community. He points out the empowering aspects of a community of oppressed people and the responsibility this community confers upon its members.
Further along these lines, Bill White has a new paper on stigma, addiction and methadone. It poses some interesting challenges to the recovering community. How do we reduce the isolation of MMT patients trying to recover? What does recovery mean in the context of MMT? "Responsibility" in the paragraph above could be interchanged with standards. One of the healing mechanisms of the recovering community is imposing standards expectations (responsibility) on its members. Would bringing MMT patients into the community erode this? (There were similar fears with psychotropics.) Does this open a door for benzos and other meds? Clearly, these standards protect the recovering community, but they also constitute a barrier.
The conundrum here is that suspicion about MMT has been pretty persistent for good reason. The paper does a good job addressing the failure of MMT in facilitating recovery. Many members of the recovering community question whether its possible for large numbers of people to achieve and maintain recovery while on methadone--if methadone is such a helpful tool and isn't a barrier to recovery, then why, with the wide distribution of methadone clinics, haven't these people been able to form their own thriving tribe within the recovering community?
It would seem that the best way to test this (the degree to which intra-group stigmatization constitutes a barrier to recovery) would be to have these folks be welcomed into the arms of the recovering community and see how they do. But, how do we get there when this suspicion persists? And, how do we respect the role of these standards in the recovering community when considering the needs of MMT patients?
This challenge is not going away.
UPDATE: Maybe expectations would have been a better choice of words than standards?

It got me thinking about some of the mechanisms of addiction and stigma, and the healing mechanisms of the recovering community. He points out the empowering aspects of a community of oppressed people and the responsibility this community confers upon its members.
Further along these lines, Bill White has a new paper on stigma, addiction and methadone. It poses some interesting challenges to the recovering community. How do we reduce the isolation of MMT patients trying to recover? What does recovery mean in the context of MMT? "Responsibility" in the paragraph above could be interchanged with standards. One of the healing mechanisms of the recovering community is imposing standards expectations (responsibility) on its members. Would bringing MMT patients into the community erode this? (There were similar fears with psychotropics.) Does this open a door for benzos and other meds? Clearly, these standards protect the recovering community, but they also constitute a barrier.
The conundrum here is that suspicion about MMT has been pretty persistent for good reason. The paper does a good job addressing the failure of MMT in facilitating recovery. Many members of the recovering community question whether its possible for large numbers of people to achieve and maintain recovery while on methadone--if methadone is such a helpful tool and isn't a barrier to recovery, then why, with the wide distribution of methadone clinics, haven't these people been able to form their own thriving tribe within the recovering community?
It would seem that the best way to test this (the degree to which intra-group stigmatization constitutes a barrier to recovery) would be to have these folks be welcomed into the arms of the recovering community and see how they do. But, how do we get there when this suspicion persists? And, how do we respect the role of these standards in the recovering community when considering the needs of MMT patients?
This challenge is not going away.
UPDATE: Maybe expectations would have been a better choice of words than standards?
Wednesday, November 04, 2009
Almost impossible to ignore
An interesting explanation of dopamine's function--distinguishing drive and motivation from pleasure and reward:

In the emerging view, discussed in part at the Society for Neuroscience meeting last week in Chicago, dopamine is less about pleasure and reward than about drive and motivation, about figuring out what you have to do to survive and then doing it. “When you can’t breathe, and you’re gasping for air, would you call that pleasurable?” said Nora D. Volkow, a dopamine researcher and director of the National Institute on Drug Abuse. “Or when you’re so hungry that you eat something disgusting, is that pleasurable?”
In both responses, Dr. Volkow said, the gasping for oxygen and the wolfing down of something you would ordinarily spurn, the dopamine pathways of the brain are at full throttle. “The whole brain is of one mindset,” she said. “The intense drive to get you out of a state of deprivation and keep you alive.”
Dopamine is also part of the brain’s salience filter, its get-a-load-of-this device. “You can’t pay attention to everything, but you want to be adept as an organism at recognizing things that are novel,” Dr. Volkow said. “You might not notice a fly in the room, but if that fly was fluorescent, your dopamine cells would fire.”
In addition, our dopamine-driven salience detector will focus on familiar objects that we have imbued with high value, both positive and negative: objects we want and objects we fear. If we love chocolate, our dopamine neurons will most likely start to fire at the sight of a pert little chocolate bean lying on the counter. But if we fear cockroaches, those same neurons may fire even harder when we notice that the “bean” has six legs. The pleasurable taste of chocolate per se, however, or the anxiety of cockroach phobia, may well be the handiwork of other signaling molecules, like opiates or stress hormones. Dopamine simply makes a relevant object almost impossible to ignore.
Tuesday, November 03, 2009
Lozenge/Patch Combo Best for Kicking Butts
Encouraging findings for people trying to quit smoking:
Placing this in the context of offering drug replacements to addicts is interesting food for thought. One important bit of context is that these were people who were trying to quit and the overarching goal of helping professionals with smokers is to try to help them quit, not reduce use. The nicotine addicts I know want full recovery. They want to be completely smoke free, and the few people I know who have been on nicotine replacement for years still really want to stop but can't. The system encourages their moves toward quitting completely and supports gradual change. That seems to be an important part of any lessons drawn from treatment for nicotine addiction. The focus of heroin maintenance is not to stabilize people while moving them toward quitting, it's to maintain them because we've concluded that they can't quit.Smokers are more than twice as likely to quit if they use the nicotine patch along with nicotine lozenges—compared to lozenges or patches alone, buproprion (Xyban), buproprion plus the lozenges or placebo. The trial was the largest study ever to compare these approaches head to head, and included 1,504 smokers.
All of the treatment groups did better than placebo—but the effect was strongest for the patch/lozenge combination, 40% of whom successfully kicked the habit. Smokers using this combo were not only more likely to quit, but also less likely to have a “slip” prompt a return to regular smoking.
The study adds support to a growing body of research that suggests that offering addicts access to drugs similar to their drug of choice—or even that drug itself—can actually help them quit or at least dramatically reduce the harm associated with their addiction.


Recovery pandemic
holy cow, it’s happening to you too.Androcles writes a nice post on the infectious nature of recovery and hope.

Substance Abuse Prevention Dollars and Cents
From a recent government report:

1.1. Costs of Substance Abuse
Studies have shown the annual cost of substance abuse to the Nation to be $510.8 billion in 1999 (Harwood, 2000). More specifically,Substance abuse clearly is among the most costly health problems in the United States. Among national estimates of the costs of illness for 33 diseases and conditions, alcohol ranked second, tobacco ranked sixth, and drug disorders ranked seventh (National Institutes of Health [NIH], 2000). This report shows that programs designed to prevent substance abuse can reduce these costs.
- Alcohol abuse cost the Nation $191.6 billion;
- Tobacco use cost the Nation $167.8 billion;
- Drug abuse cost the Nation $151.4 billion.
1.2. Savings From Effective School-Based Substance Abuse Prevention
If effective prevention programs were implemented nationwide, substance abuse initiation would decline for 1.5 million youth and be delayed for 2 years on average. It has been well established that a delay in onset reduces subsequent problems later in life (Grant & Dawson, 1997; Lynskey et al., 2003). In 2003, an estimated:The average effective school-based program in 2002 costs $220 per pupil including materials and teacher training, and these programs could save an estimated $18 per $1 invested if implemented nationwide. Nationwide, full implementation of school-based effective programming in 2002 would have had the following fiscal impact:
- 5.6 percent fewer youth ages 13–15 would have engaged in drinking;
- 10.2 percent fewer youth would have used marijuana;
- 30.2 percent fewer youth would have used cocaine;
- 8.0 percent fewer youth would have smoked regularly.
Substance Abuse Prevention Dollars and Cents: A Cost-Benefit AnalysisAlthough 80 percent of American youth reported participation in school-based prevention in 2005 (SAMHSA, 2004), only 20 percent were exposed to effective prevention programs (Flewelling et al., 2005).
- Saved State and local governments $1.3 billion, including $1.05 billion in educational costs within 2 years;
- Reduced social costs of substance-abuse-related medical care, other resources, and lost productivity over a lifetime by an estimated $33.7 billion;
- Preserved the quality of life over a lifetime valued at $65 billion.
Massive, Risky and Expensive
Mark Kleiman responds to pushback on some of his alternatives to incarceration:

The suggestion that various non-punitive programs might control crime, and that doing so was preferable, ceteris paribus, to controlling crime by inflicting damage on offenders, met with an especially furious response, mostly centered on the phrase “liberal social engineering.” But the project of putting 1% of the adult population behind bars — an incarceration rate five times as high as any other advanced democracy, and five times as high as the U.S. ever had before 1975 — is itself a massive, massively risky, and expensive social-engineering project, and no less massive, risky, or expensive for never having been thought through. It also involves a completely unprecedented expansion of the power of the state over the individual.If all taxation is theft, then the $200 billion required to support the current policing, adjudication, and corrections systems is just as much “stolen” as the much smaller sums that might be usefully expended on improving parental performance by poor young first-time mothers, removing lead from the environment, or improving classroom discipline. If people who call themselves fiscal conservatives understood that a sentence of life without parole imposed on an 18-year-old represented a present-value expenditure of $1 million, the enthusiasm for “throwing away the key” might be diminished. (An execution, including the due process required — but not sufficient — to prevent the execution of the innocent, costs more.)
In my view, crime at current levels is such a social problem that even substantial increase in the $200 billion criminal-justice budget would be justified by even modest decreases in crime. If we can spend an extra $10 billion a year to have reduced crime and reduced incarceration, so much the better.
Now for the specifics:
1. Evidence about the capacity of nurse-family partnerships to reduce offending by more than 50% (based on a randomized controlled trial) is here.
2. Evidence about the impact of lead on crime takes two forms: individual-level studies, and econometric studies. The results are consistent, and the effect sizes are large. Moreover, the biology is understood: lead, even at low levels, damages cognitive function, and lower-level cognitive functioning reduces deterrability, thus increasing crime. Moreover, lead does specific damage to impulse control.
Therefore, lead causes crime, and removing lead reduces crime. It does so more cost-effectively than increasing incarceration, and it has side-benefits rather than side-costs.
3. I have no doubt that a minimum legal drinking age of 21 reduces drinking among minors, and that relaxing that rule would increase drinking (and drinking-related problems) in that population. It also generates massive disobedience and the mass acquisition of false ID. Increased alcohol taxes are effective in reducing drinking, and especially in reducing heavy, problem drinking (since an extra tax of a dime a drink wouldn’t much bother someone who averages a drink a day). The biggest impacts are on heavy drinking by minors, whose incomes tend to be limited. A combination of relaxing the age restriction and raising the price could reduce heavy drinking while avoiding the criminalization of mass behavior.
British Drug Classification
Andrew Sullivan offers a clear and concise summary of the an initiative to reclassify drugs (the classifications are used to determine criminal penalties).
Take the question of alcohol and tobacco out of the discussion and it seems quite sensible. Add alcohol and tobacco back and you have a firestorm. Is this about being too soft on drugs, or is this about protecting the status of alcohol and tobacco?

Take the question of alcohol and tobacco out of the discussion and it seems quite sensible. Add alcohol and tobacco back and you have a firestorm. Is this about being too soft on drugs, or is this about protecting the status of alcohol and tobacco?
Wounded Systems of Care
We spend a lot of time talking about recovery-oriented systems of care. Important, but should we first look at facilitating recovery for our systems of care?
Peapod writes about healing treatment systems (systems, not clients). She draws from a recent Bill White document about the Philadelphia experience and describes a critical juncture:

Peapod writes about healing treatment systems (systems, not clients). She draws from a recent Bill White document about the Philadelphia experience and describes a critical juncture:
In Philadelphia in 2004, they decided to tackle the things that were wrong in their services. They did a giant exercise in information gathering, something they called a ‘fearless inventory’ after the AA fourth step. You can see the detail here:
They uncovered that some unhealthy stuff was going on. Organisations were not talking to each other. They existed like islands connected by drawbridges that ‘were permanently up’.
Focus groups uncovered “an underlying tone of paternalism, disrespect and, at times, outright contempt.”
Sunday, November 01, 2009
The right sentence
The Washington Post looks toward the end of the crack/powder cocaine sentencing disparity with some ambivalence. It appears that they failed to consider whether prison sentences are an effective tool for addressing the harm associated with crack use.
IN THE 1980s, entire communities were devastated by the addiction and violence that accompanied crack, a smokable form of cocaine. Congress reacted by passing extraordinarily tough laws, including one that mandated a minimum prison sentence of five years for those in possession of as little as five grams of crack. Those arrested with 50 grams were automatically slapped with a 10-year sentence.
This supposed solution, backed at the time by many in the Congressional Black Caucus, turned out to be destructive also. Tens of thousands of black men -- many of them first-time offenders with no history of violent crime -- found themselves behind bars for inordinately long periods. White and Hispanic offenders -- those most often collared for powder cocaine violations -- had to be caught with 100 times the amount of powder to trigger the same mandatory minimum sentences.
. . .
smoking crack delivers a faster, more intense high than snorting powder and that this high is more short-lived, thus compelling most crack users to seek additional doses of the drug. The differences in addiction rates between crack and powder are not enormous, but they are real, and the study also notes that crack users often experience faster rates of physical deterioration than do those who consume powder. The report notes that roughly one-fourth of crack offenders are associated with violence, and that this rate exceeds that for powder cocaine offenders. As in the 1980s, predominantly African American communities continue to bear the brunt of the crime and addiction brought on by this awful drug.
These facts suggest that there should be some difference in the penalties for crack and powder cocaine, but how much? This is a difficult question to answer with precision, so perhaps the best solution would be to eliminate the mandatory minimums for both crack and powder and build into the sentencing guidelines tougher penalty ranges for crack that judges could apply on a case-by-case basis
Saturday, October 31, 2009
A reality check on drug use
George Will recently wrote a column on drug policy:
The Economist magazine says this means that more than 200 million people -- almost 5 percent of the world's adult population -- take illegal drugs, the same proportion as a decade ago. The annual U.S. bill for attempting to diminish the supply of drugs is $40 billion. Of the 1.5 million Americans arrested each year on drug offenses, half a million are incarcerated. "[T]ougher drug laws are the main reason why one in five black American men spend some time behind bars," the Economist said in March.
"There is no correlation between the harshness of drug laws and the incidence of drug-taking: citizens living under tough regimes (notably America but also Britain) take more drugs, not fewer." Do cultural differences explain this? Evidently not: "Even in fairly similar countries tough rules make little difference to the number of addicts: harsh Sweden and more liberal Norway have precisely the same addiction rates."
The good news is the progress America has made against tobacco, which is more addictive than most illegal drugs. And then there is alcohol.
In "Waking Giant: America in the Age of Jackson," historian David S. Reynolds writes that in 1820, Americans spent on liquor a sum larger than the federal government's budget. By the mid-1820s, annual per capita consumption of absolute alcohol reached seven gallons, more than three times today's rate. "Most employers," Reynolds reports, "assumed that their workers needed strong drink for stimulation: a typical workday included two bells, one rung at 11 a.m. and the other at 4 p.m., that summoned employees for alcoholic drinks."
The elderly Walt Whitman said, "It is very hard for the present generation anyhow to understand the drinkingness of those years. . . . it is quite incommunicable." In 1842, a Springfield, Ill., teetotaler named Lincoln said that liquor was "like the Egyptian angel of death, commissioned to slay, if not the first, the fairest born in every family." Which helps explain why the nation sobered up (somewhat -- these things are relative). One reason crack cocaine use has declined is that a generation of inner-city young people saw what it did to their parents and older siblings.
Undoubtedly culture changes are critical to changing these behaviors, though it's my understanding that one reason for those high rates of alcohol consumption was that alcoholic beverages were often safer to drink than the available water.
I'd like to better understand how that culture change happened. Can it occur without heavy moralizing and the formation of temperance societies? It would seem that this culture change eventually culminated in prohibition. Clearly not what George Will has in mind.
Bacon, cheesecake and Ho Hos, oh my!
Not sure what to make of this:
Junk food elicits addictive behavior in rats similar to the behaviors of rats addicted to heroin, a new study finds. Pleasure centers in the brains of rats addicted to high-fat, high-calorie diets became less responsive as the binging wore on, making the rats consume more and more food. The results, presented October 20 at the Society for Neuroscience’s annual meeting, may help explain the changes in the brain that lead people to overeat.
“This is the most complete evidence to date that suggests obesity and drug addiction have common neurobiological underpinnings,” says study coauthor Paul Johnson of the Scripps Research Institute in Jupiter, Fla.
It will be interesting to watch this research unfold. I worry about the the meaning of addiction as a brain disease being rendered meaningless by an ever-growing list of behaviors that are associated changes in the pleasure centers and dopamine production and response. I look forward to comparative research of these brain responses to better understand the differences.
Sunday, October 25, 2009
Committed to treatment
Anchorage, AK is taking some very aggressive steps to address public drunkenness in their community:
Though court coerced treatment is common, commitment to treatment is unusual. Discussion of these matters in papers and blogs suggest we have two options: 1) harm reduction approaches that accept the person as they are, emphasize personal liberty and make no attempt to address the root cause of their suffering; or 2) lock-em up.
I suppose this approach represents a third way in these too often polarized debates and I suppose that's laudable. The cases discussed in the video and story clearly are seriously endangering themselves. However, the coercion involved in this approach should make everyone uncomfortable. I have a few thoughts about that.

The new mayor, Dan Sullivan, a Republican, has created a staff position and a task force devoted to addressing homelessness. The police recently gained the authority to dismantle homeless encampments with just 12 hours’ notice. Citizen groups are patrolling parks where homeless camps have been the site of rapes and other violence. But in perhaps the biggest and most controversial break from how the city has handled the problem in the past, a Salvation Army detoxification and alcohol abuse treatment center has begun accepting chronic inebriates who have been taken there essentially by force.There is also a video about the story here.
With $1.2 million in new state financing pushed through by one of Alaska’s more liberal Democrats, State Senator Johnny Ellis of Anchorage, the facility, the Clitheroe Center, is accepting people committed under a state law, Title 47. Under the law, a judge can order people into secure treatment for 30 days, and potentially for months, if the police, a doctor or family members convince the judge that the person’s abuse of alcohol has made them a threat to themselves and others. The person does not need to have committed a crime.
“Ten years ago, there would have been a community outcry that Johnny Ellis is locking up people with the disease of addiction,” Mr. Ellis said. “ ‘How can he do that and say he’s still a progressive?’ ”
Now, Mr. Ellis said, the problem has increased so much “that for various motivations people are saying let’s try something new.” He added, “The people dropping dead during the summertime really got this community paying attention.”
One homeless person drowned. Another was hit by a car. One died from hypothermia. Most had been drinking, and several had four or even five times the blood-alcohol level above which a person is considered too drunk to drive. Experts say the problem of public drunkenness is part of a larger homeless problem that disproportionately affects Native Alaskans, particularly men who have moved in from rural parts of Alaska and lost their way in the city. The recession has also played a role.
Involuntary commitment of homeless alcoholics has been used elsewhere in the country. Some homeless advocates say it infringes on civil rights, and they question its effectiveness. Here in Anchorage, several longtime advocates said the severity of the situation had made them open to giving it a chance.
Though court coerced treatment is common, commitment to treatment is unusual. Discussion of these matters in papers and blogs suggest we have two options: 1) harm reduction approaches that accept the person as they are, emphasize personal liberty and make no attempt to address the root cause of their suffering; or 2) lock-em up.
I suppose this approach represents a third way in these too often polarized debates and I suppose that's laudable. The cases discussed in the video and story clearly are seriously endangering themselves. However, the coercion involved in this approach should make everyone uncomfortable. I have a few thoughts about that.
- First, I'm skeptical of slippery slope arguments. Sometimes the slippery slope is the right place to be.
- The ethics of this seem to rest on questions of free will in addiction. If one believes the addict is not free, coercive interventions make sense. (More here, here, here, here, here, here and here.)
- Adopting this positive view of liberty opens the door to potential abuses by the state. Coercion should be a last resort.
- Attraction is preferable. This problem is not just a problem of individuals with a disease. It's likely a symptom of a system failure. Does a recovery-oriented system exist? One that encompasses the complete continuum from harm reduction to long term drug free treatment and recovery support? What if we added Project SAFE style recovery coaches engaged in aggressive outreach? Help support a vibrant recovering community that was capable of transmitting infectious hope and continuous peer support? How many could we attract voluntarily?
- That an alternative to palliative care and coercion exists, means that those would be justifiable only if voluntary attraction into recovery failed, or as a stopgap while implementing a voluntary system.
- This approach would require investing in more than just the squeaky wheels. It would mean investing in the well-being and recovery of all addicts.
Friday, October 23, 2009
Tab dump
- A brief history of scholastic inebriation (Too bad they missed Robert Smith whose U of M fraternity brothers called his father to fetch him because his drinking was out of hand.)
- Claims injection site dropped Downtown Eastside crime 'very much exaggerated,' say cops
- Battling Addiction With Those Who Know It Best
- New UK study suggests minimal relationship between cannabis and schizophrenia or psychosis
- Cocaine exposure during pregnancy leads to impulsivity in male, not female, monkeys




Medical Marijuana Take Down
Chuck Lane writes a two post take down on medical marijuana.
As turned off as I am by anything that includes the word "druggie", he more or less states my position. Personal drug possession should be among the lowest enforcement priorities and should not result in incarceration. If there is or was a legitimate medical marijuana movement it's been co-opted by people whose goal is decriminalization of recreational use--a defensible position but a dishonest approach to achieving it. Finally, this just isn't the way we do medicine.

As turned off as I am by anything that includes the word "druggie", he more or less states my position. Personal drug possession should be among the lowest enforcement priorities and should not result in incarceration. If there is or was a legitimate medical marijuana movement it's been co-opted by people whose goal is decriminalization of recreational use--a defensible position but a dishonest approach to achieving it. Finally, this just isn't the way we do medicine.
Wednesday, October 21, 2009

Tuesday, October 20, 2009
Same info, different reactions
I wonder what this means for addiction recovery and treatment messaging:

A study that will appear in the December issue of the American Journal of Public Health tracked the ways in which party affiliation related to people's responses to identical information on diabetes.
Participants in the study read a mock news article on the American Diabetes Association lobbying Congress for greater attention to Type 2 diabetes, the sixth-leading cause of death in the United States. Some people read a straight news report, with minimal mention of what causes diabetes. Others read one of three versions of the story: one that pegged the disease primarily to genetic factors; one that emphasized personal choices; and one that focused on social and environmental factors, such as access to safe places to exercise and affordable, healthy food.
The study's authors, University of Pennsylvania researcher Sarah E. Gollust, along with the University of Michigan's Paula M. Lantz and Peter A. Ubel, were most interested in how people responded to the notion that "social determinants" -- how easy it is to buy fresh vegetables or exercise, among other things -- are underlying causes of disease. Public health advocates have been promoting the importance of these factors, believing that the more people know about these circumstances, the more likely they are to want to help.
But that assumption doesn't hold up. When people who identified themselves as Democrats read specifically about the social factors that can lead to Type 2 diabetes, they expressed greater backing for public health policies aimed at addressing those factors; Republicans, by contrast, registered much lower levels of support.
"The take-home message is that people can walk away from the same information with different attitudes," Gollust says.
Sunday, October 18, 2009
A tough approach to drug-using mothers
The LA Times paints a pretty sympathetic picture of Project Prevention, a program that pays addicticted women to get themselves sterilized or use long term birth control. It closes with the following:
This is pessimism and stigma dressed up as compassion. It only reinforces the notion that addicts are hopeless, irresponsible social parasites. Indeed, the founder has previously said, "We don’t allow dogs to breed. We spay them. We neuter them. We try to keep them from having unwanted puppies, and yet these women are literally having litters of children …" She also previously distributed flyers saying, "Don't let getting pregnant get in the way of your drug habit."
I'm all for preventing unwanted pregnancies, but context matters. If this group was also lobbying for greater access to treatment for these women, that might be another matter. They give lip service to the welfare of the women but little more. Their statistics report only on the social costs of the addicts and offers no references to anything the program has done to improve the circumstances of the women--even activities like advocacy and treatment referrals which would cost nothing and be easy to track. One can only assume that they don't engage in these kinds of activities, collect data and report on it because they and their supporters don't care.

Project Prevention makes sense to me. Although a few thousand IUDs might not make a dent in the problem, the bluntness of the gesture turns up the volume.It doesn't "make a dent in the problem" but it "turns up the volume." Turns up the volume of what exactly? Bringing them "in on the dialogue"? Who's dialogue? "Helping mothers heal" by encouraging sterilization?
And it brings drug-using moms in on the dialogue. Thank you for helping me do the first responsible thing I've ever done with my addiction, one mother wrote in a letter to Harris, who solicits a life story from every client.
"They're not bad women," Harris told me. "They don't set out to have babies that are taken away. They feel regret about what they've done."
She's right. Demonizing the mothers doesn't help. They need counseling, not just contraception. Many were victims of childhood trauma and are prisoners of addiction now.
Some hope giving birth will redeem and stabilize their lives. "It's one of the few things they can do that they have control over," said retired social worker Glynis Morrow. "Then the realities of parenting hit. And they feel like failures. And that pain drives them back to drugs."
And we're right back where we started from.
So we can talk about women's rights or about the privilege of procreation. However we cast the conversation, there is one truth we can't avoid: We are helping mothers heal when we keep unwanted children from being born.
This is pessimism and stigma dressed up as compassion. It only reinforces the notion that addicts are hopeless, irresponsible social parasites. Indeed, the founder has previously said, "We don’t allow dogs to breed. We spay them. We neuter them. We try to keep them from having unwanted puppies, and yet these women are literally having litters of children …" She also previously distributed flyers saying, "Don't let getting pregnant get in the way of your drug habit."
I'm all for preventing unwanted pregnancies, but context matters. If this group was also lobbying for greater access to treatment for these women, that might be another matter. They give lip service to the welfare of the women but little more. Their statistics report only on the social costs of the addicts and offers no references to anything the program has done to improve the circumstances of the women--even activities like advocacy and treatment referrals which would cost nothing and be easy to track. One can only assume that they don't engage in these kinds of activities, collect data and report on it because they and their supporters don't care.
Saturday, October 17, 2009

Treatment reduces criminal recidivism
Not surprising:

The 2009 Annual Report of the Office of Substance Abuse Treatment Services (OSATS), formerly the Division of Addiction and Recovery Services, includes return-to-custody data on offenders who paroled in Fiscal Year 2005-06 for a one-year and a two-year period. The return to custody rate after one year for offenders completing both in-prison and community-based treatment in FY 2005-06 was 21.9 percent compared to 39.9 percent for all offenders. The return to custody rate after two years for offenders completing both in-prison and community-based treatment in FY 2005-06 was 35.3 percent compared to 54.2 percent for all offenders.
For male offenders, the return-to-custody rate after one year for those who completed both in-prison and community-based substance abuse treatment in FY 2005-06 was 25.4 percent compared to 41.2 percent of all male offenders. The return-to-prison rate after two years for male offenders who completed both in-prison and community-based substance abuse treatment in FY 2005-06 was 40.4 percent compared to 55.6 percent of all male offenders.
Female offenders were especially responsive to substance abuse treatment. After one year, only 8.8 percent of female offenders who completed both in-prison and community-based substance abuse treatment in FY 2005-06 were returned to custody compared to 30.1 percent of all female offenders. The return-to-prison rate after two years for female offenders who completed both in-prison and community-based substance abuse treatment in FY 2005-06 was 16.5 percent compared to 43.7 percent of all female offenders.
GAIN publications
The Lighthouse Institute has compiled all the publications based on GAIN data (Dawn Farm uses the GAIN in adolescent services). They have full text articles for many of them.
Very cool. Thanks Lighthouse!

Very cool. Thanks Lighthouse!
Friday, October 09, 2009
Students for Recovery @ University of Michigan
Thanks Ivana. It's been needed for years.

For many students, moving to Ann Arbor to begin their careers at the University of Michigan is a time of excitement, curiosity and maybe a little bit of fear. But for School of Social Work graduate student Ivana Grahovac, the emotions were different.Read the rest here.
As Grahovac prepared to start her time at the University, she was also recovering from a five-year addiction to heroin. Though she had been clean and sober for four-and-a-half years in her hometown of Bloomfield Hills, Mich., she wasn’t sure she could recreate that security in Ann Arbor.
Grahovac said coming to Ann Arbor was a “leap of faith” and that once she arrived, she felt her sobriety constantly threatened.
“I was constantly getting these e-mails about being invited to join people for keggers, drink night specials and pub-crawls,” she said. “There was just a real lack of understanding going on that maybe there are people for whom this would be a very bad choice and possibly cause some serious negative and tragic consequences to occur.”
It was in this environment that Grahovac decided to create Students for Recovery, a group aiming to support and provide provides information for students recovering from addiction. The group also helps students find sober programming as an alternative to the usual Friday night party filled with red Solo cups and alcohol.
Tuesday, October 06, 2009
A dishonest political agenda
From the Honorary President of the International Harm Reduction Association (page 8) [via PeaPod]:
If so, great. We're on the same side. If not, stop giving lip service to helping people who use drugs stop.
As a recovery advocate that is thousands of miles away, I see a frustrating parallel with discussions here. The HR advocates adopt a hyper-rational posture, denying that their values are reflected anywhere in their beliefs and practice while accusing recovery advocates of being close scientific cousins of intelligent design advocates.
What evidence do recovery advocates ignore? There is ample evidence that we can be as effective at treating addiction as we are with other chronic diseases like hypertension, diabetes and asthma. Should we reject the current treatments for those too?
Why is it undeliverable financially? Because the public doesn't support it? Isn't that the point of advocacy? Why quash advocacy work that is focused on improving the lives of the people you also advocate for? Why not collaborate to make sure a complete continuum is offered?
One other observation. Mr. O'Hare did not the use of the word addiction or any its variants. Does that intimate something? It may be nothing (Really, I mean that.), but it make me wonder if he's invested in framing as something other than a disease.
[hat tip: PeaPod]

I am completely in favour of helping people who use drugs to stop, if that is what they want. I assume that is what is meant by ‘recovery’. Working with anyone who has problems with drugs must start where the individual is and could involve a range of strategies. Harm reduction should permeate the services available to drug users, which should be used on the basis of evidence of effectiveness, including cost-effectiveness, and on the basis of allocating scarce resources in the most effective way on a population base.I wonder about the evidence for his first statement. How many people has he or his organization helped achieve drug-free recovery? How many of the people they serve want drug-free recovery, and how many people can't access services to achieve this goal? Do they track this information? Do they use it to advocate for more drug-free treatment services?
If so, great. We're on the same side. If not, stop giving lip service to helping people who use drugs stop.
The recovery agenda is a dishonest political agenda, by which some treatment agencies are positioning themselves for a seamless transition to a Conservative government. It ignores evidence and relies on faith. It is becoming evangelistic. It is dishonest because it is completely undeliverable financially and it raises false hopes. It is not a public health approach.Whoa! I'm not there to see for myself, so I don't know if the U.K. recovery movement is a cabal of political conservatives or ideologues trying to exploit political conservatives. I see no political pandering on Wired in.
As a recovery advocate that is thousands of miles away, I see a frustrating parallel with discussions here. The HR advocates adopt a hyper-rational posture, denying that their values are reflected anywhere in their beliefs and practice while accusing recovery advocates of being close scientific cousins of intelligent design advocates.
What evidence do recovery advocates ignore? There is ample evidence that we can be as effective at treating addiction as we are with other chronic diseases like hypertension, diabetes and asthma. Should we reject the current treatments for those too?
Why is it undeliverable financially? Because the public doesn't support it? Isn't that the point of advocacy? Why quash advocacy work that is focused on improving the lives of the people you also advocate for? Why not collaborate to make sure a complete continuum is offered?
The basis of drugs work should always be harm reduction. It should always be public health-based and if it helps with public order that is fine with me.Why is drug-free treatment incompatible with public health? I think it is, but it's also important to keep in mind some of the limitations of public health models--tension between prevention and treatment is common in these arguments, Public health approaches always include the application of some values (even when we say they don't), and they risk turning life and death decisions for entire classes of people into cold accounting exercises. For example, why do we cringe at a harm reduction/public health approach to female circumcision? (More here and here.)
One other observation. Mr. O'Hare did not the use of the word addiction or any its variants. Does that intimate something? It may be nothing (Really, I mean that.), but it make me wonder if he's invested in framing as something other than a disease.
[hat tip: PeaPod]
Friday, October 02, 2009
It's not on the list!!!
Mark Kleiman being interviewed about his new book. This segment focuses on drug policy:

A civil rights movement
Powerful language from wired in to recovery:

Many people would argue that the UK treatment system, in main, is simply managing symptoms and accepting long-term disability or discomfort of people with serious substance use problems.
These same people would not argue against the value of treatment per se, rather it needs to be provided in a different way.
The recovery movement is first and foremost a civil rights movement. It is about helping disadvantaged people, people with problems, improve their well-being.
It is about helping people with substance use problems (and often many other problems) reclaiming or claiming their right to a safe, dignified, meaningful and gratifying life in the community, sometimes despite their problems.
A recovery oriented system of care places the person with the problem at the centre of the system. It does not just build places where people go and get ‘treatment’ – it builds forms of support theroughout the community.
It accepts that the struggles of the person are not just with what is going on within their own body and mind – it is about their social struggles, which they experience because of the prejudice, discrimination, stigma and marginalisation that occurs in society.
Alcohol marketing and teen drinking
The finding from a study of the relationship between alcohol advertising and adolescent alcohol use:

Based on the consistency of findings across the studies, the confounders controlled for, the dose response relationships, as well as the theoretical plausibility and experimental findings regarding the impact of media exposure and commercial communications, it can be concluded from the studies reviewed that alcohol marketing increases the likelihood that adolescents will start to use alcohol, and to drink more if they are already using alcohol.
"Recovery is recovery"
Bill White interviews a medication assisted recovery advocate:
[via dailydose.net]

The problem with the methadone community is we have too many people who think methadone is a magic bullet for that disease—that recovery involves nothing more than taking methadone.He bemoans the lack of recovery-oriented providers:
This view is reinforced by people who, with the best of intentions, proclaim, “Methadone is recovery.” Methadone is not recovery. Recovery is recovery. Methadone is a pathway, a road, a tool. Recovery is a life and a particular way of living your life. Saying that methadone is recovery let’s people think that, “Hey, you go up to the counter there, and you drink a cup of medication, and that’s it. You’re in recovery.” And of course, that’s nonsense. Too many people in the methadone field learn that opiate dependence is a brain disorder, and they think that that’s all there is to it. But just like any other chronic medical condition, it has a behavioral component that involves how you live your life and the daily decisions you make.
Bill: Do you see the methadone clinics in the United States developing more recovery-oriented philosophies in their service practices?This will be a very interesting movement to watch. Read the rest here.
Walter: I wish I could say I did, but it’s a yes and no. I’ve been to all the AATOD conferences since 2001 and there are clearly people who are developing more recovery-oriented programs, but there are 1200 methadone programs in the U.S. How many are represented at the AATOD? 40? So yes, some of the programs are developing more recovery-oriented services, but many are not.
[via dailydose.net]
Thursday, October 01, 2009

In 16 states, drug deaths overtake traffic fatals
From the Washington Post:
Read the rest here.

In 16 states and counting, drugs now kill more people than auto accidents do, the government said Wednesday.
Experts said the startling shift reflects two opposite trends: Driving is becoming safer, and the legal and illegal use of powerful prescription painkillers is on the rise.
Read the rest here.
Another reason to quit smoking
Phillip-Morris played a role in killing health care reform in 1994:

Whatever your feelings about health care reform, is this the kind of interest we want secretly manipulating the debate?McCaughey's lies were later debunked in a 1995 post-mortem in The Atlantic, and The New Republic recanted the piece in 2006. But what has not been reported until now is that McCaughey's writing was influenced by Philip Morris, the world's largest tobacco company, as part of a secret campaign to scuttle Clinton's health care reform. (The measure would have been funded by a huge increase in tobacco taxes.) In an internal company memo from March 1994, the tobacco giant detailed its strategy to derail Hillarycare through an alliance with conservative think tanks, front groups and media outlets. Integral to the company's strategy, the memo observed, was an effort to "work on the development of favorable pieces" with "friendly contacts in the media." The memo, prepared by a Philip Morris executive, mentions only one author by name:
"Worked off-the-record with Manhattan and writer Betsy McCaughey as part of the input to the three-part exposé in The New Republic on what the Clinton plan means to you. The first part detailed specifics of the plan."
McCaughey did not respond to Rolling Stone's request for an interview.
Monday, September 28, 2009
21 reduces alcohol dependence
More evidence for the argument that lowering drinking ages would lead to more alcohol and drug problems later in life. The point about age of first use vs. regular use is interesting and offers some interesting questions about goals and strategies for prevention programming.

UPDATE: Oops. Here's the link.Background: Many studies have found that earlier drinking initiation predicts higher risk of later alcohol and substance use problems, but the causal relationship between age of initiation and later risk of substance use disorder remains unknown.
Method: We use a "natural experiment" study design to compare the 12-month prevalence of Diagnostic and Statistical Manual, Fourth Edition, alcohol and substance use disorders among adult subjects exposed to different minimum legal drinking age laws minimum legal drinking age in the 1970s and 1980s. The sample pools 33,869 respondents born in the United States 1948 to 1970, drawn from 2 nationally representative cross-sectional surveys: the 1991 National Longitudinal Alcohol Epidemiological Survey (NLAES) and the 2001 National Epidemiological Study of Alcohol and Related Conditions. Analyses control for state and birth year fixed effects, age at assessment, alcohol taxes, and other demographic and social background factors.
Results: Adults who had been legally allowed to purchase alcohol before age 21 were more likely to meet criteria for an alcohol use disorder [odds ratio (OR) 1.31, 95% confidence intervals (95% CI) 1.15 to 1.46, p < 0.0001] or another drug use disorder (OR 1.70, 95% CI 1.19 to 2.44, p = 0.003) within the past-year, even among subjects in their 40s and 50s. There were no significant differences in effect estimates by respondent gender, black or Hispanic ethnicity, age, birth cohort, or self-reported age of initiation of regular drinking; furthermore, the effect estimates were little changed by inclusion of age of initiation as a potential mediating variable in the multiple regression models.
Conclusion: Exposure to a lower minimum legal purchase age was associated with a significantly higher risk of a past-year alcohol or other substance use disorder, even among respondents in their 40s or 50s. However, this association does not seem to be explained by age of initiation of drinking, per se. Instead, it seems plausible that frequency or intensity of drinking in late adolescence may have long-term effects on adult substance use patterns.
Sunday, September 27, 2009
The Sunday ritual
I'm not much of Mitch Albom fan, but good for him. Whether one agrees with him or not, it's something we all take for granted and it deserves discussion.

The video featured two attractive women.
It was shot by an onlooker.
It hit YouTube by storm.
You're no doubt thinking "sex," but let me assure you the women kept their clothes on. Unfortunately, that was the only ladylike thing about them.
On the video, they appeared intoxicated, swore like sailors, got in fights, then screamed, shoved and cursed until security finally took them away, one in handcuffs.
This was not a women's penitentiary. It was a Lions game. You can argue that watching the Lions might make anyone go ballistic. But I'm guessing these women, like many football fans, had another reason for their belligerence:
They were hammered before the game began.
And you could shoot this video every Sunday.
Look, it's bad enough that most NFL games begin at 1 p.m. and that people are buying beers before kickoff. But thanks to tailgating, many fans are blotto before they hand over their tickets. One day, we'll explain to Martians our tradition of arriving hours before a football game, sitting in cold parking lots in fold-up beach chairs, swigging beers and grilling fatty foods between bumpers of pickups (at which point the Martians will bolt to their spaceships).
...
I blame the tailgaters, but I also blame the teams -- pro and college. By encouraging a seven-hour drinking experience, football now sees its stadiums marred with behavior like this past week's wildly popular YouTube moment (billed as "Two Drunk Girls Kicked out of Vikings vs Lions Game").
Saturday, September 26, 2009
Highlights from the conference "How AA and NA Work"
Presentations (hopefully video too) will be up next week. I'll post a link when they're up.
Sarah Zemore gave a great presentation on the evidence for the effectiveness of 12 step groups. It was powerful and well organized. I found a link to an identical presentation here.
She very effectively rebutted the Cochrane Review from a few years ago by making the following points. (These are based on notes I took and are incomplete. Hopefully they post video so that you can see her complete rebuttal for yourself.)
Laudet made one self-evident point that jarred me because it is almost never made in professional circles. She pointed out that the subjects of one of her studies were infected with HIV at a rate of 22% and Hep C at a rate of 33%. She then said something to the effect of, "As a public health matter, we need to focus on keeping these people in recovery. If they relapse they are likely to spread these illnesses."
When's the last time you read anything about recovery as a strategy to reduce communicable disease?
Laudet (as did Zemore) attempted to deconstruct AA, so that it's mechanisms for change could be identified and still be offered to clients who prefer not to participate in AA or NA.
Bill White gave a rousing historical perspective of AA and NA's histories and pointed out the looming challenges that face twelve-step recovery groups. These challenges included matters like methadone maintenance patients as full NA members and the limitations of the 3rd tradition and singleness of purpose in AA. He noted that fewer that 18% of people entering treatment in the U.S. were primarily identified as alcohol dependent.

Sarah Zemore gave a great presentation on the evidence for the effectiveness of 12 step groups. It was powerful and well organized. I found a link to an identical presentation here.
She very effectively rebutted the Cochrane Review from a few years ago by making the following points. (These are based on notes I took and are incomplete. Hopefully they post video so that you can see her complete rebuttal for yourself.)
- It was limited only to randomized trials and ignored the overwhelming observational evidence.
- It included one of Zemore's studies which was NOT a randomized study of AA.
- She acknowledged that the randomized evidence is ambiguous.
- Randomized trials of AA are hard to do because some subjects in other groups end up participating in AA. This happened in Project MATCH.
- The Cochrane Review did not find Twelve-step Facilitation ineffective. It found it no more effective that CBT and MET.
- Finally, she cited 4 randomized studies of Twelve-step Facilitation: The outpatient arm of Project MATCH, a study by her colleague Kaskutas, and two others that I missed.
Laudet made one self-evident point that jarred me because it is almost never made in professional circles. She pointed out that the subjects of one of her studies were infected with HIV at a rate of 22% and Hep C at a rate of 33%. She then said something to the effect of, "As a public health matter, we need to focus on keeping these people in recovery. If they relapse they are likely to spread these illnesses."
When's the last time you read anything about recovery as a strategy to reduce communicable disease?
Laudet (as did Zemore) attempted to deconstruct AA, so that it's mechanisms for change could be identified and still be offered to clients who prefer not to participate in AA or NA.
Bill White gave a rousing historical perspective of AA and NA's histories and pointed out the looming challenges that face twelve-step recovery groups. These challenges included matters like methadone maintenance patients as full NA members and the limitations of the 3rd tradition and singleness of purpose in AA. He noted that fewer that 18% of people entering treatment in the U.S. were primarily identified as alcohol dependent.
Thursday, September 24, 2009
How AA/NA Work
The University of Michigan will host a conference tomorrow on How AA/NA Work and will stream it live here. The presenters include some very big names. Here's the agenda:

Friday, September 25, 2009
9:00 am - 4:00 pm
| 09:00-09:20 | Introductions by John Traynor and Bob Zucker |
| 09:20-10:00 | Alcoholics Anonymous Effectiveness: Faith Meets Science by Sarah Zemore, PhD, Scientist, Alcohol Research Group, Public Health Institute |
| 10:00-10:40 | Twelve-step participation among polydrug users: Longitudinal patterns, effectiveness, and (some) lessons learned by Alexandre B. Laudet, Ph.D., Director, Center for the Study of Addictions and Recovery (C-STAR) and Deputy Director of the Institute for Treatment and Services Research, National Development and Research Institute |
| 10:40-11:00 | BREAK |
| 11:00-11:40 | The Varieties of recovery experience: AA, NA and the diversification of pathways and styles of long- term addiction recovery by William L. White, M.A., Senior Research Consultant, Chestnut Health Systems / Lighthouse Institute. Author of: Slaying the Dragon - The History of Addiction Treatment and Recovery in America |
| 11:40-12:20 | From iPod to iGod: Are 12-step Groups Hip Enough for Adolescents? by John F. Kelly, Ph.D., Associate Director, Mass. General Hospital/Harvard Center for Addiction Medicine, Director, Addiction Recovery Management Service (ARMS) at Mass. General Hospital, Assistant Professor of Psychiatry, Harvard Medical School |
| 12:20-01:30 | LUNCH |
| 01:30-02:10 | Alcoholics' perceptions of AA's helpfulness: Qualitative responses and association with drinking outcomes by Elizabeth A. R. Robinson, MSW, Ph.D., Research Assistant Professor, at the University of Michigan Department of Psychiatry Substance Abuse Section |
| 02:10-02:30 | BREAK |
| 02:30-04:00 | Panel Discussion |
Cause, effect & underage drinking
Two interesting findings about underage drinking. The first on the relationship between early alcohol use and chronic alcohol problems later in life. The second looks at the relationship between early alcohol use and poor judgment later in life.
We've known for some time that there is a relationship between early drinking and alcohol problems later in life. What's been unclear is the nature of that relationship. Does early exposure to alcohol cause changes in the adolescent brain that lead to problems later in life? Does early exposure facilitate the expression of genes that are related to alcoholism? These two theories would suggest that early exposure to alcohol has the potential to cause alcohol problems later in life. Or, is early exposure an indicator of risk factors such as the environment the young person is in or risk taking behavior? These would suggest that there is no causal relationship.
A new study supports the gene expression theory:

We've known for some time that there is a relationship between early drinking and alcohol problems later in life. What's been unclear is the nature of that relationship. Does early exposure to alcohol cause changes in the adolescent brain that lead to problems later in life? Does early exposure facilitate the expression of genes that are related to alcoholism? These two theories would suggest that early exposure to alcohol has the potential to cause alcohol problems later in life. Or, is early exposure an indicator of risk factors such as the environment the young person is in or risk taking behavior? These would suggest that there is no causal relationship.
A new study supports the gene expression theory:
On the second matter, Scientific American [via 3 Quarks Daily] suggests that there is a causal relationship between early exposure to alcohol and poor judgement long after the effects of the alcohol wear off:Background: Research suggests that individuals who start drinking at an early age are more likely to subsequently develop alcohol dependence. Twin studies have demonstrated that the liability to age at first drink and to alcohol dependence are influenced by common genetic and environmental factors, however, age at first drink may also environmentally mediate increased risk for alcohol dependence. In this study, we examine whether age at first drink moderates genetic and environmental influences, via gene × environment interactions, on DSM-IV alcohol dependence symptoms.
Methods: Using data on 6,257 adult monozygotic and dizygotic male and female twins from Australia, we examined the extent to which age at first drink (i) increased mean alcohol dependence symptoms and (ii) whether the magnitude of additive genetic, shared, and nonshared environmental influences on alcohol dependence symptoms varied as a function of decreasing age. Twin models were fitted in Mx.
Results: Risk for alcohol dependence symptoms increased with decreasing age at first drink. Heritable influences on alcohol dependence symptoms were considerably larger in those who reported an age at first drink prior to 13 years of age. In those with later onset of alcohol use, variance in alcohol dependence was largely attributable to nonshared environmental variance (and measurement error). This evidence for unmeasured gene × measured environment interaction persisted even when controlling for the genetic influences that overlapped between age at first drink and alcohol dependence symptoms.
Conclusions: Early age at first drink may facilitate the expression of genes associated with vulnerability to alcohol dependence symptoms. This is important to consider, not only from a public health standpoint, but also in future genomic studies of alcohol dependence.
It's no secret that binge drinking and faulty decision-making go hand in hand, but what if poor judgment lingered long after putting the bottle down and sobering up? A new study with rats suggests that heavy alcohol consumption in adolescence could put people on the road to risky behavior.(U.W.) in Seattle fed alcohol to a group of rats and found that their ability to make good decisions was impaired even long after they stopped consuming booze.
Several studies have associated heavy drinking in youth with impaired judgment in adulthood, but these studies didn't resolve whether alcohol abuse actually predisposes people to develop bad decision-making skills, or if the people who indulged in excessive inebriation were risk-taking types to begin with. As Selena Bartlett, a director in the Ernest Gallo Clinic and Research Center at the University of California, San Francisco, explains, you cannot put adolescents in a room and ask them to consume alcohol to see what happens. But scientists can conduct these kinds of experiments with rats, an animal that Bartlett, who was not part of the study, says is "excellent for modeling changes in behavior" as a result of alcoholism.
In the new study published this week in Proceedings of the National Academy of Sciences, scientists at the University of Washington
Tuesday, September 22, 2009
Harm Reduction Defined
From the International Harm Reduction Association:
[via drugscope]

‘Harm Reduction’ refers to policies, programmes and practices that aim primarily to reduce the adverse health, social and economic consequences of the use of legal and illegal psychoactive drugs without necessarily reducing drug consumption. Harm reduction benefits people who use drugs, their families and the community.Not bad for a definition developed by a committee.
[via drugscope]
Sunday, September 20, 2009
Ending the war on drugs does not equal legalization
An interesting take on the growing chorus of calls to end the war on drugs.
The first problem I have with the op-ed is that she conflates ending the drug war with legalization, offering an fallacious binary choice. The piece is a hard sales pitch for her position.
She offers 2 reasons for these calls:
She goes on to make a humanitarian case based on the suffering in the developing world. Ironically, Antonio Maria Costa makes a humanitarian case against legalization based on the suffering it would cause in developing world.

The first problem I have with the op-ed is that she conflates ending the drug war with legalization, offering an fallacious binary choice. The piece is a hard sales pitch for her position.
She offers 2 reasons for these calls:
Two significant developments are contributing to the sudden surge in calls for reconsidering prohibition. The first is that drugs are now damaging long-term Western security interests, especially in Afghanistan and Mexico. The second is that production is migrating away from its traditional homes like Colombia and the Golden Triangle and moving into the heart of Western consumer areas like Canada, the Netherlands and Britain.I don't have a global perspective, but, in the US, it seems to me that domestic policy is driving the reconsideration of drug policy. One factor is moral, the insane incarceration rates for drug offenders (From the early 1980s to the to the early 2000s, the number of inmates whose worst offense was a drug crime grew by 1540% in federal prisons and 1195% in state prisons.) The other is financial, with state budgets buckling under the recession and the cost of incarcerating all these people.
She goes on to make a humanitarian case based on the suffering in the developing world. Ironically, Antonio Maria Costa makes a humanitarian case against legalization based on the suffering it would cause in developing world.
He ends with the same kind of hard sell, resorting to an appeal to classism.At the moment, fewer than 5% of all adults in the world take drugs at least once a year, compared with around one-quarter who smoke tobacco and about a half who drink alcohol. Drugs kill about 200,000 people a year, tobacco 5 million and alcohol 1.8 million. Why open the floodgates to addiction by increasing access to drugs? Would the world really be a better place with a lot more people under the influence of drugs?
John Gray seems to think so. In last week's Observer he argued that the case for legalising all drugs is unanswerable. Yet who would answer for the havoc wrought on the vulnerable? Maybe western governments could absorb the health costs of increased drug use, if that's how taxpayers want their money to be spent.
But what about the developing world? Why unleash an epidemic of addiction in parts of the world that already face misery, and do not have the health and social systems to cope with a drug tsunami?
Critics point out that vulnerable countries are the hardest hit by the crime associated with drug trafficking. Fair enough. But these countries would also be the hardest hit by an epidemic of drug use, and all the health and social costs that come with it. This is immoral and irresponsible.
Let's be open-minded about how to improve drug control. But let's do it in a way that will improve the health and safety of our communities and not just make it easier for City bankers and high-street models to snort cocaine.
Friday, September 18, 2009
Monday, September 14, 2009
9 components of recovery
David Clark at wiredin.org.uk expounds on a list of 9 components of recovery from the mental health recovery movement. They are:

- Renewing hope and commitment to one’s life
- Being supported by others
- Finding one’s niche in the community
- Redefining self or changing one’s identity
- Incorporating illness
- Managing symptoms.
- Assuming control
- Fighting stigma
- Being an empowered citizen

More on Mexico's drug policy reform
Five opinions on Mexico's recent move to decriminalize possession.
Too hot, too cold, just right...
They also make irreconcilable statements of fact.
Here are some of the highlights:

Too hot, too cold, just right...
They also make irreconcilable statements of fact.
Here are some of the highlights:
...if they asked me, will decriminalization of the possession of small amounts of drugs save a single life in Ciudad Juárez, where there have been about 3,200 murders in 21 months, my answer would be a rotund no.Grrrr:
But decriminalizing drug possession is in and of itself a change of, paradoxically, gigantic and modest proportions. Gigantic because it is a solid first step to pave the way for 1) distinguishing between drug use and drug abuse 2) paving the way for fully medicalizing abuse, that is, reinforcing the idea that we should treat drug addicts much as alcoholics and offer them help instead of prison time, and 3) focusing state resources on the production, trafficking and distribution networks. But modest because it still commits governments to continue their war on drugs, just not on the user.
Drug users are not innocent. They support the vicious drug cartels. Without their demand for drugs, the supply side has no purpose. Since terrorists depend on the drug market to fund their activities, users are potentially aiding terrorism. Because drug traffickers are frequently linked with weapons and human trafficking, users are also supporting these activities.

Subscribe to:
Posts (Atom)